



Single Anastomosis Duodenal Switch (SADI) – What Can You Expect from the New Bariatric Surgery Device?

by Walter Medlin, MD, FACS
Spring 2021
The disease of obesity is never cured and each weight-loss operation has different effects and outcomes for everyone. Genetics, medications and other health issues can lead to differences in weight-loss or weight regain with the exact same operation. Everyone’s body is different and because of that, results from weight-loss operations will vary.
With weight-loss operations sometimes being unpredictable or having negative side effects, there is a constant need to improve bariatric surgery and make it more effective. In an attempt to do this, the single anastomosis duodeno-iliostomy (SADI) was created.
What is SADI?
SADI is a simplified duodenal switch that only bypasses 60 to 75% of the small bowel. Anastomosis means one connection instead of two, which is what separates this surgery from the regular duodenal switch. Normally, the regular duodenal switch has two major steps:
- The first step is a sleeve gastrectomy in which about 80% of the stomach is removed, leaving a smaller tube-shaped stomach that is similar to a banana.
- The second step bypasses the majority of the intestine by connecting the end portion of the intestine to the duodenum near the stomach. A BPD/DS limits how much you can eat and reduces the absorption of nutrients, including proteins and fats.
With SADI, while there are two parts, there is only one connection. The duodenal switch contains two connections. SADI makes the surgery less demanding on the surgeon and can reduce potential bowel twisting later. It has about the same safety as surgery, but is much more effective for weight control and for diabetes control.
How is SADI Performed?
SADI has two parts:
- The upper part of the stomach is just a sleeve, which leaves a tubular stomach instead of a broad, floppy stomach.
- The lower half can be done at the same time but can also be done later and involves the surgeon dividing the duodenum (upper most part of the small bowel). The upper portion of the divided duodenum is now plugged in to the small bowel further downstream, usually 2/3 to 3/4 of the way down. This allows food to go directly into the lower bowel and bypass the rest of your bowel.
This bypassed bowel is not completely inactive and is also not removed. The bypassed bowel now allows for bile to come through, which sweeps out any bacteria. The bile can now join the food at the point where the upper duodenum is now plugged in and digestion can occur. Because the duodenum and upper small bowel no longer see any of the food you eat, this radically changes some of the signals that they normally make.
Below the connection point where food and bile is now joined, a lot of work has to happen that used to happen far upstream! This makes a big difference in how the gut signals the brain because it usually does not have that much work to do.
Essentially, this process changes your gut-brain signals and leads to less hunger and more time feeling full. Most people even notice a change in food cravings or pickiness.
Why Does SADI Work?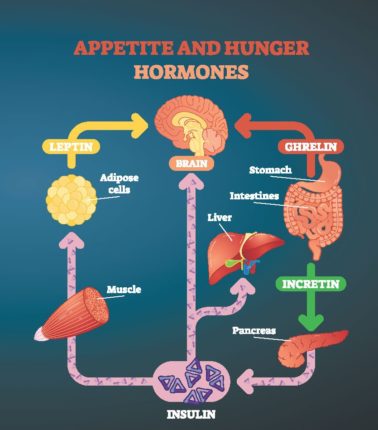
All of our current operations mostly work by changing the signals from the gut and fat tissue that the brain interprets as “low energy.” Normally, when our brain feels low on energy, we become hungry. The goal is to change the hunger and fullness signals.
There are many different “signal” hormones from the bowel, including:
- Leptin from fat – alters food intake and controls energy
- Ghrelin from the stomach – increases food intake
- PYY – communicates to your brain that you are full and decreases your appetite
- GIP – stimulates insulin secretion
- GLP1 –helps regulate appetite after eating
- CCK – stimulates digestion of fat and protein
Even though sleeve gastrectomy only changes the stomach, it does have some impact on these signals.
Bypass operations like the gastric bypass and duodenal switch modify these other signals more. The duodenal switch gives the largest impact on the most number of signals. Now, SADI has the same impact on those signals but in a modified surgery.
Since we are all different in terms of our genes, you can see how some people might be more responsive to an operation that hits more signals, while other people may do great with just a change in Ghrelin. How our brain adapts over time to these different signals is not any indication of how hard we are working at weight management. There’s plenty of room to take personal responsibility without spiraling into shame, blame or comparing.
So, Why Hasn’t SADI Taken Over the World?
First, the gastric sleeve bariatric surgery is such an awesome procedure for most people that there is no reason to jump to SADI right away.
Second, and more important, is that surgeons are very slow to change to any new operation, and most of us are not really trained to divide the duodenum. It is not super hard to learn, but there are a few very important structures in the area that we have to take extreme care around. Most of us in training only got into this area when it was in the middle of a terrible disease, like cancer or injury or bleeding, and we have never really been there when it is well-behaved! When things go bad in the area, they tend to go really bad, and surgeons are not wrong to have great respect for the duodenum.
Third, the older, original version of the duodenal switch was much more problematic and got a bad reputation for loose bowel movements and severe malnutrition. SADI has addressed and improved most of these shortcomings for most people.
Fourth, we are still in an era of insurance craziness, and the duodenal switch and SADI are no exception. Both of our national and international surgical organizations recognize SADI as a standard of care. They are scientifically and medically well-established. Insurance companies usually drag their feet even in the face of science, though. The good news is that if you have sleeve coverage under your insurance, an upgrade later to SADI is usually less than $10,000 or $12,000, even if you have to pay for it out of pocket. Coverage can usually be obtained for the upgrade, so don’t lose hope.
Take Away Points
In 2021, gastric bypass should only be done when absolutely medically needed. Otherwise, the risks are normally too high. The sleeve definitely has some known issues but can be easily modified and is almost never a bad choice, even if it may not be the end of the story. SADI is the version of the duodenal switch that is almost always appropriate, and it is worth it for you to find a surgeon who offers it if you want to find out more about your individual care.
About the Author:
Walter Medlin, MD, FACS, is a bariatric surgeon in Salt Lake City, Utah and Lehi, Utah. He performs mostly sleeve gastrectomy and SADI/loop duodenal switch operations, and revision surgeries at Bariatric Medicine Institute. He is a grateful member of the Obesity Action Coalition (OAC) and supports his patients with the OAC Chairman’s Council program sponsored memberships. He had sleeve gastrectomy in 2008 and upgraded to SADI in 2019. He had a revision of this in late 2020 and is doing well! Dr. Medlin LOVES to play outside, especially paragliding and kitesurfing. You can find his YouTube channel at “BMIUtah” and “Walter Medlin.”
Check out the video below of our author, Dr. Medlin, taking a deep dive into SADI!

by Kendall Griffey, OAC Communications Manager Spring 2024 We have officially kicked off Your Weight Matters Regional…
Read Article
by OAC Staff Members Kendall Griffey and Michelle “Shelly” Vicari Winter 2024 In a world that often…
Read Article
by Rachel Engelhart, RD; Kelly Donahue, PhD; and Renu Mansukhani, MD Summer 2023 Welcome to the first…
Read Article