



Obesity and Age


by Julie DeJean Marks, MEd, LCES
Winter 2011
Does obesity have the same effects on kids as it does on adults? There are definitely age-related determinants.
Among the adult population affected by obesity, poor self-image and self-esteem are very common. One study (Strauss, 1999) found that in children affected by obesity, their self-esteem does not differ significantly from a child not affected by obesity up to ages nine or 10. In fact, according to the Center on an Aging Society, “children affected by obesity seem as socially well-adjusted and are just as likely to be happy as children not affected.” As children age and begin to develop their social image, they begin to rely more on their peers for their sense of identity and social support.
The Effects of Obesity on Children Versus Adults
In June 2004, a review of literature was done by the Texas Department of Health to determine the effects of childhood obesity. Both short and long-term effects on financial status, psychological and physiological factors were noted. Children affected by obesity may experience bullying in all forms, such as teasing, name calling and physical harm. They are often the subject of rumors and/or lies and experience social isolation due to rejection by their peers.
These experiences frequently cause damaging effects to their self-esteem as well as emotional distress and anxiety along with other psychological disorders such as depression, suicidal thoughts and extreme dieting (anorexia/bulimia).
Adults who have been affected by obesity since childhood and developed low self-esteem are more likely to face discrimination in educational settings and the workplace, thus achieving lower educational status. They are also less likely to marry. A greater decrease in activity, including walking, shopping, attending movies and parties and increased feelings of sadness and hopelessness are found in adults between the ages of 51 to 69.
Health Effects of Obesity
Health problems typically found in adults are becoming increasingly common in children, such as hypertension (high blood pressure), type 2 diabetes and increased risk of heart disease. Also, increased stress on the joints may eventually lead to structural problems by early adulthood.
Obesity increases the risk of developing many chronic and even fatal conditions. Along with the more obvious, including high blood pressure, coronary heart disease, diabetes and stroke, there is also a higher risk of cancer.
Decreased mobility and inability to perform activities of daily life, such as eating, bathing and dressing, are common among older individuals affected by obesity. These adults frequently suffer from persistent and chronic symptoms of illness such as fatigue, breathing problems, depression and increased symptoms of arthritis and joint problems. In fact, the effects of obesity on chronic conditions are comparable to the physiological effects of approximately 20 years of aging.
Preventing the Effects of Obesity
Can the effects of obesity be prevented? In one study, (Mellin et al, 2002) good family connections protected children against the adverse effects of obesity. With children, parental support and communication can positively affect self-esteem and lead to increased participation in group activities and improved social relationships. As well, participation in group or team activities is also associated with improved social skills and self-esteem. Children with obesity are more likely to remain affected by obesity throughout their adult life (Wing, Koeske, & Valoski, 1987), and the population with obesity increases with age (Lohman, 1987).
Basal Metabolic Rate (BMR) and its Role in Obesity
The number of adults with obesity has increased rapidly since 1991 and is much higher among the age population of 51 to 69. A variety of things contribute to obesity as age progresses and even during childhood, however, the main factor is a slower metabolism or basal metabolic rate (BMR).
BMR is the total amount of energy that the body uses on a daily basis to stay alive and function. With age, people move less which slows metabolism. The decrease in movement is due in part to responsibilities, but mainly because of technology which is also a major factor in childhood obesity.
Through technology, less activity is required to perform basic tasks, such as turning on the television or the lights and washing dishes and clothes. Video games and computers have also drawn people away from outside activities.
With age and a decrease in activity, muscle tissue, which is a major source of energy production, begins to get smaller and fewer calories are burned on a daily basis due to the decreased metabolism. If foods with large amounts of calories are consumed as well, then the body will quickly gain weight. Muscle mass can be maintained and/or improved through an increase in physical activity which slows the progression of aging. Consuming smaller portions of nutritionally sound foods contributes to a higher metabolism.
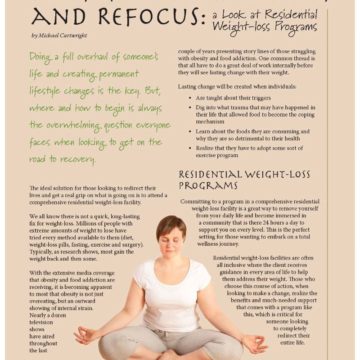
Conclusion
Metabolism is controlled by the individual and can be adjusted up or down, kind of like a thermostat, by the lifestyle one chooses. When the metabolism is raised through activity and proper nutrition, an increase in energy level will result. Energy is produced in the body in the form of heat; therefore, with increased metabolism a person is less likely to feel cold and begins to sweat sooner after activity has begun. As metabolism increases and the body becomes more efficient, a lower heart rate may be noticed. However, these effects will diminish quickly in just a few days of inactivity and poor nutrition.
A healthy lifestyle must be consistently maintained for life and is more easily maintained when established during childhood.
About the Author:
Julie DeJean Marks, MEd, LCES, is a clinical exercise physiologist, licensed by the state of Louisiana. She received her master’s degree in exercise physiology from the University of Houston in 1991 and has been certified by the American College of Sports Medicine as an exercise test technologist and a clinical exercise specialist. Julie is currently counseling bariatric patients on exercise at Lafayette General Medical Center in Lafayette, LA.
References:
Strauss RS Dieting and self-reported weight status among young adolescents. Arch Child Adolesc Med 1999; 153:741-747
Strauss, Richard S., MD, Childhood Obesity and Self-Esteem, Journal of the American Academy of Pediatrics, Pediatrics, Electronic Article, Vol 105, No. 1, January, 2000, p. e15.
Lohman, T. G. (1987). The use of skinfolds to estimate body fatness on children and youth. Journal of Physical Education, Recreation & Dance, 58(9), 98-102. EJ 364 412.
Epstein, L. H., Wing, R. R., Koeske, R., & Valoski, A. (1987). Long-term effects of family-based treatment of childhood obesity. Journal of Consulting and Clinical Psychology, 55(1), 91-95. EJ 352 076.
Mellin AE, Neumark-Sztainer, D., Story, M. et al., {a} Unhealthy behaviors and psychosocial difficulties among overweight adolescents. The potential impact of familial factors. Journal of Adolescent Health (2002); 31: 145-153
Center on an Aging Society, Georgetown University, Data Profile: Obesity Among Older Americans, No. 10, July 2003
https://www.weightlossforall.com/losing-weight-age.htm
https://www.weightlossforall.com/metabolic-changes-age-x.htm
https://www.weightlossforall.com/metabolism-signs-raised.htm
Related Resources

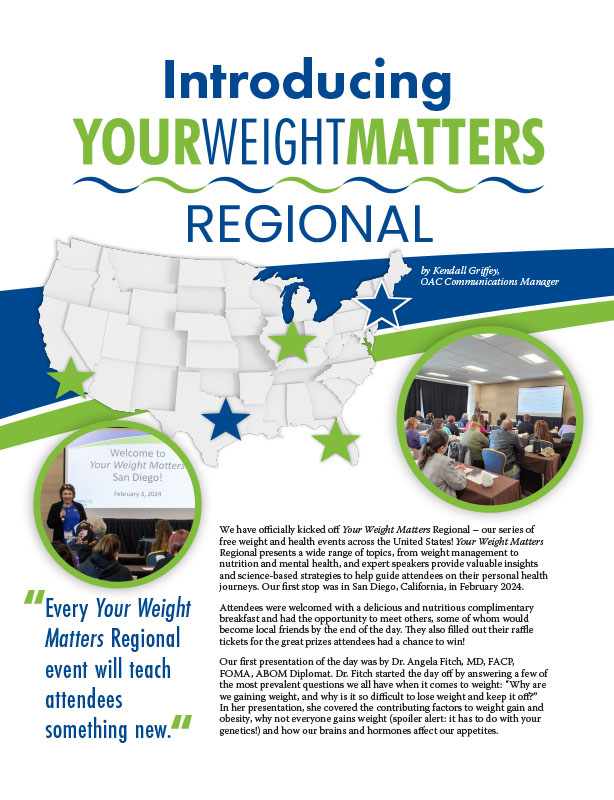
by Kendall Griffey, OAC Communications Manager Spring 2024 We have officially kicked off Your Weight Matters Regional…
Read Article
by Michelle “Shelly” Vicari Winter 2024 Winter has arrived! Don’t allow the chilly and damp weather to…
Read Article
by Kendall Griffey, OAC Communications Coordinator Winter 2024 The Obesity Action Coalition’s 12th annual Your Weight Matters…
Read Article